

Protein-calorie malnutrition is a form of malnutrition that arises as a result of insufficient intake of protein and/or energy (calories). This condition is usually secondary to debilitating diseases such as advanced cancer, AIDS.
Protein-caloric malnutrition in cancer
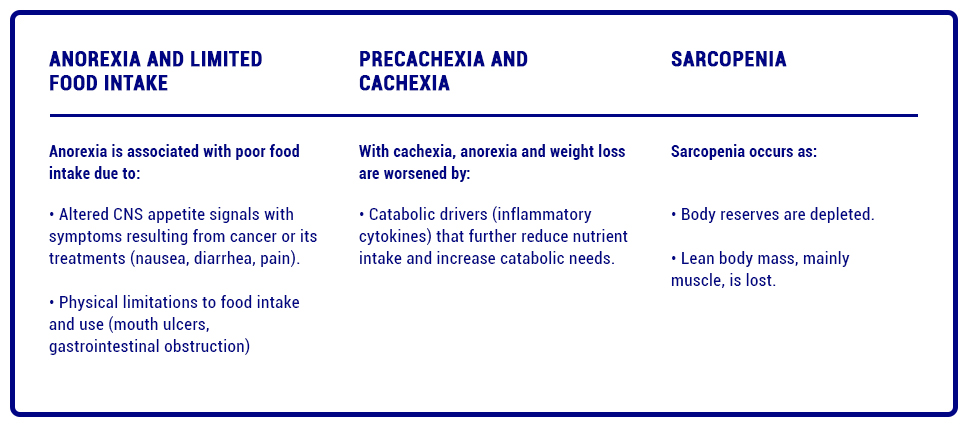
Cancer patients are at particularly high risk of malnutrition as a result of the disease itself and its treatments. On the one hand, the disease results in metabolic changes that are driven by proinflammatory cytokines and tumor-derived factors leading to anorexia-cachexia syndrome.
In addition to metabolic changes driven by the proinflammatory state and tumor, pain and other factors associated with the disease and its treatment such as gastrointestinal tract obstructions, dysphagia, depression, drug effects, can significantly limit oral intake, affecting nutritional status and driving the progression of cachexia and sarcopenia.
It is estimated that 10-20% of deaths in cancer patients can be attributed to malnutrition rather than the malignancy itself.[1][2][3]
Studies on body composition of cancer patients reveal that, specifically, skeletal muscle loss with or without fat loss is the main aspect of cancer-associated malnutrition that predicts the risk of physical deterioration, postoperative complications, chemotherapy toxicity, and mortality. Nutritional counseling along with oral nutrition supplementation (ONS) is recommended as an effective strategy to preserve lean mass.[4]
According to ESPEN guidelines 25-30 kcal/kg/day with 1.2 to 1.5 g protein/kg/day serve as a target range to help maintain or restore lean body mass; it has been proposed that even higher doses of protein may be necessary when depletion is severe. [4][5]
Protein-calorie malnutrition in HIV/AIDS.
On the other hand, malnutrition is a threat to people living with HIV/AIDS. There are different mechanisms that explain weight loss such as:
-
- Reduction of caloric-protein intake
-
- Increase in nutrient losses
-
- Increased metabolic expenditure
The decrease in protein-calorie intake is multifactorial and is given by factors such as anorexia, vomiting, dysphagia, intestinal obstruction, depression and altered level of consciousness.
Increased nutritional losses could happen because:
-
- Malabsorption (caused by enteropathy-HIV, intestinal pathogens, Kaposi’s sarcoma, intestinal lymphoma, drugs and malnutrition itself, which causes hypoalbuminemia and produces structural and functional alterations of the intestine).
-
- Diarrhea (50% of AIDS patients).
The increase in spending given by the presence of fever, infection, respiratory failure, cardiac failure, inflammation and certain endocrine disorders.[6]
Multiple effects caused by malnutrition in different organs and systems have been described:
-
- Skeletal muscle: Atrophy of muscle fibers = Loss of strength and decreased resistance to effort.
-
- Skin and pharynx: Thinning and loss of skin elasticity, and in more advanced stages erythematous, atrophic and hyperpigmented areas. Increased susceptibility to bedsores. Delayed wound healing. Thinning and dry hair, with greater tendency to fall out. Brittle and grooved nails due to growth disorders.
-
- Cardiovascular: Decrease in cardiac mass. Decreased cardiac index. Conduction disorders. Decreased intravascular volume. Decreased O2 consumption in fasting and increased in aggression syndrome.
-
- Liver: Hepatic steatosis.
-
- Endocrine functions: Altered insulin levels (decreased in fasting, increased in aggression syndrome). Decreased thyroid hormones in fasting, increased in aggression syndrome. Primary gonadal dysfunction (amenorrhea).
-
- Kidney: Decreased urine density and polyuria. Variations in glomerular filtration rate due to changes in cardiac output. Loss of urinary acidification capacity and metabolic acidosis.
-
- Respiratory system: Pulmonary structural changes, decreased pulmonary surfactant, loss of diaphragm mass, alteration of ventilation control mechanisms with decreased ventilatory response to hypoxia.
-
- Gastrointestinal tract: Decreased production of secretory IgA, villous atrophy and decreased barrier function against infections.
-
- Immunological consequences: Not only large variations, but small magnitudes of weight loss can influence immune function.
Nutritional intervention in malnourished patients with wasting diseases.
International management guidelines propose nutritional interventions for people with these conditions in order to prevent
with these conditions in order to prevent deterioration of health and favor the efficacy of treatments.
treatments.

Nutrisite® Polymeric is a food for medical purposes, indicated for the nutritional treatment of adults with protein-calorie malnutrition and/or sarcopenia associated with cachexia secondary to debilitating diseases such as AIDS or advanced cancer. Read more